Healthcare Is the #1 Cause of Death — and It’s Not Even Close
The medical system’s own data admits it.
The biggest threat to patient safety isn’t external disease—it’s the medical system itself.
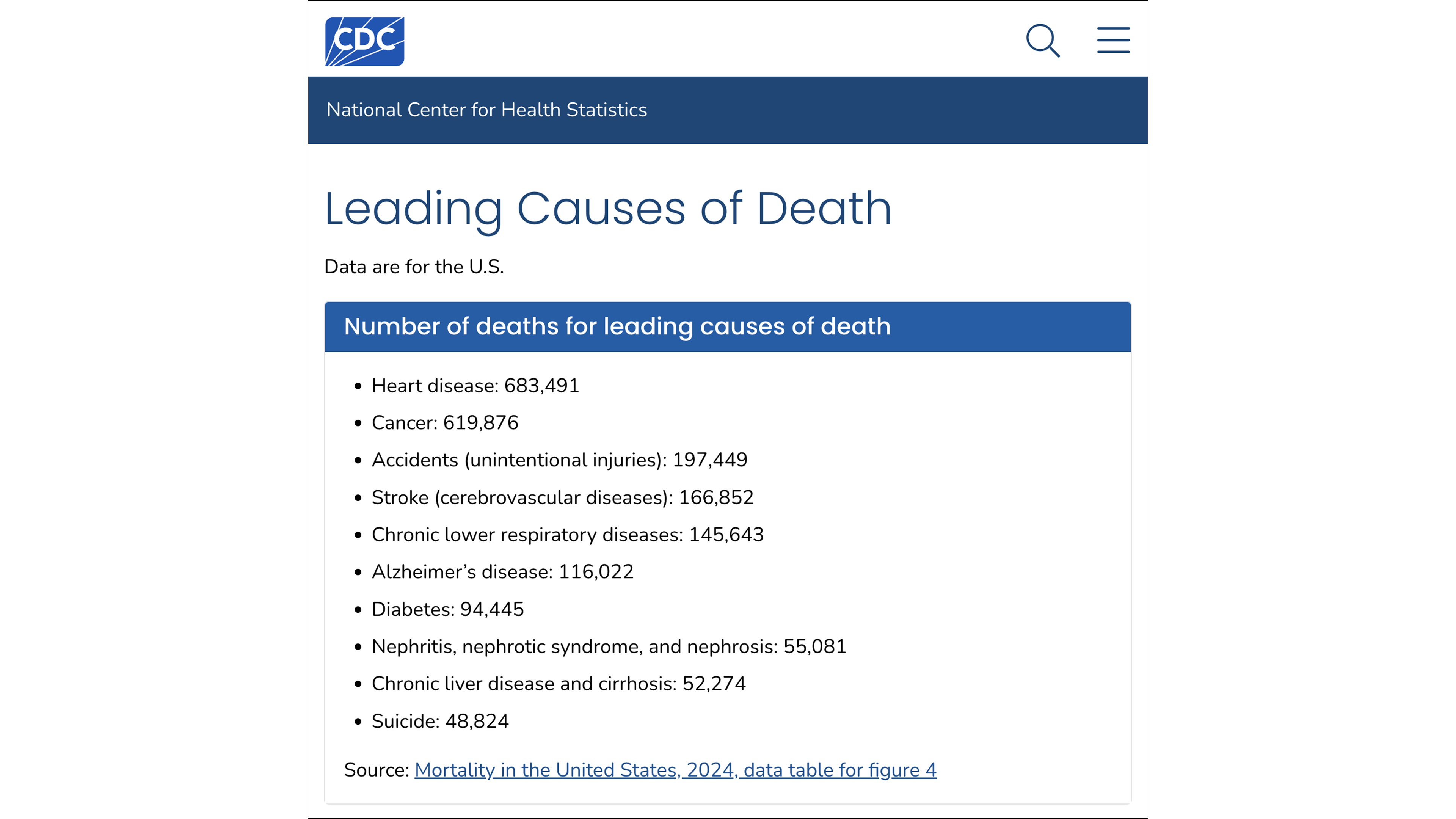
If you search for the “leading causes of death” in the United States, you will be directed to CDC data listing heart disease and cancer at the top—healthcare-related deaths aren’t even included on the list. But those statistics come from death certificates and ICD codes (International Classification of Diseases) that are structurally incapable of recording the massive number of deaths caused by the medical system.
How the medical system launders the deaths it causes
The CDC’s mortality statistics run on ICD codes that don’t properly track the medical system’s own failures. When a doctor or a pharmaceutical drug kills a patient, the cause is recorded as a biological endpoint—such as cardiac arrest or organ failure—and grouped under broader categories like heart disease or cancer, effectively erasing the medical system’s culpability in the death.
The scale of this erasure is massive. A 2000 study in The American Journal of Medicine compared two federal databases and found a 34-fold difference: the FDA’s own reporting system captured many more adverse drug reactions than were recorded on official death certificates—and it is those dramatically lower death certificate numbers that feed the CDC’s mortality rankings.
It’s a self-reinforcing feedback loop. The deaths the medical system causes inflate the very disease categories used to justify the treatments that caused them.
When you move past the official death certificates and into the audits conducted by the system’s own researchers, you find that healthcare is the leading cause of death
Half a million deaths per year: the bare minimum
The medical system kills at least half a million people in the United States every year—a figure derived from the system’s own data that represents only the absolute floor of a death toll that is, in reality, much larger. This figure is an extremely conservative synthesis of data published in the world’s most prestigious medical journals—including JAMA, The BMJ, and research from institutions like Johns Hopkins.
This death toll is compiled from distinct, non-overlapping categories of harm—ranging from medical errors to adverse reactions from properly prescribed medication. The researchers behind these papers emphasize that these are conservative estimates, and that the true scale of mortality is much higher.
I. Inpatient medical errors (>250,000 deaths per year)
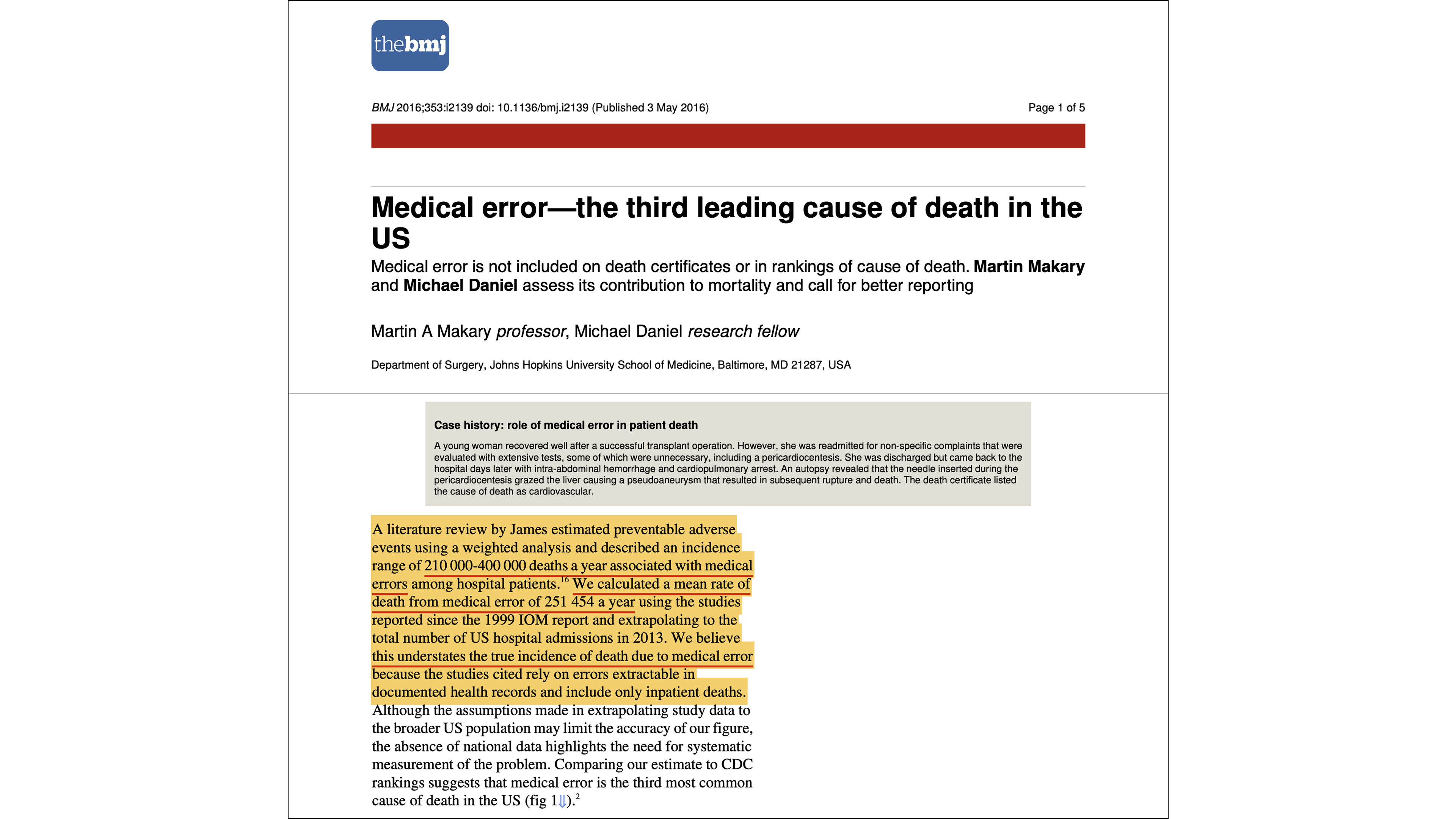
At least 250,000 patients in the United States die in the hospital setting every year due to medical errors. These include errors of commission (harmful action), errors of omission (failing to provide necessary care), communication breakdowns (ineffective or missing information sharing), contextual errors (disregarding the patient’s life circumstances), and diagnostic errors (missed, delayed, or incorrect diagnoses).
The benchmark for this 250,000+ figure is systemic mortality models, namely a 2016 Johns Hopkins study published in The BMJ, which calculated a rate of 251,454 deaths per year due to medical errors by meta-analyzing decades of patient safety research. This estimate is corroborated by a 2013 analysis in the Journal of Patient Safety, which identified objective clinical triggers—such as unplanned returns to the operating room or sudden cardiac arrest in low-risk patients.
Critics will cite lowballed estimates for deaths due to medical errors, such as a 1999 Institute of Medicine (IOM) report (44,000–98,000 deaths) or a 2020 Yale meta-analysis (~22,000 deaths). These estimates are derived from physician reviews and an overly narrow threshold for establishing causation. This physician-review model is prone to institutional bias and systematically underestimates deaths. Doctors naturally want to protect their own profession, so reviewers typically default to blaming a patient’s illness for a death, even when a colleague’s error was the catalyst. By measuring only the most obvious, singular acts of negligence rather than the preventable failure of the entire hospital system, the physician-review model significantly underestimates the true death toll of inpatient care.
II. Inpatient medication reactions (>125,000 deaths per year)
Over 125,000 patients in the United States die in the hospital setting every year due to adverse reactions from pharmaceutical drugs that were properly prescribed and followed. This category is distinct from medical errors; these are not procedural mistakes, but deaths caused by the inherent toxicity and unpredictable pharmacology of drugs deemed “safe” for clinical use.
The foundation for this death toll was first established by a 1998 JAMA meta-analysis (106,000 deaths) and further substantiated in 2013 by a paper in the Journal of Law, Medicine & Ethics, which calculated a baseline of 128,000 inpatient deaths per year. The researchers behind the 128,000 figure emphasized that this represents a significant undercount, noting that structural issues—like the FDA’s prioritization of rapid drug approval over long-term safety monitoring—leave tens of thousands of additional deaths unaccounted for.
This death toll is compounded by the modern explosion of polypharmacy, where the standard of care increasingly involves prescribing multiple medications to manage the side effects of other medications. With over a quarter of adults in the U.S. now taking four or more prescription drugs daily, we have created a medical environment where the risk of fatal drug interactions has climbed dramatically—yet remains invisible to mortality monitoring systems.

III. Outpatient deaths (>100,000 deaths per year)
The medical system’s least-measured—and likely largest—category of fatalities occurs outside hospital walls. These deaths, at home or in nursing facilities, escape all oversight: no charts are reviewed, no root cause analyses are triggered, and no questions are asked about the role of medical intervention.
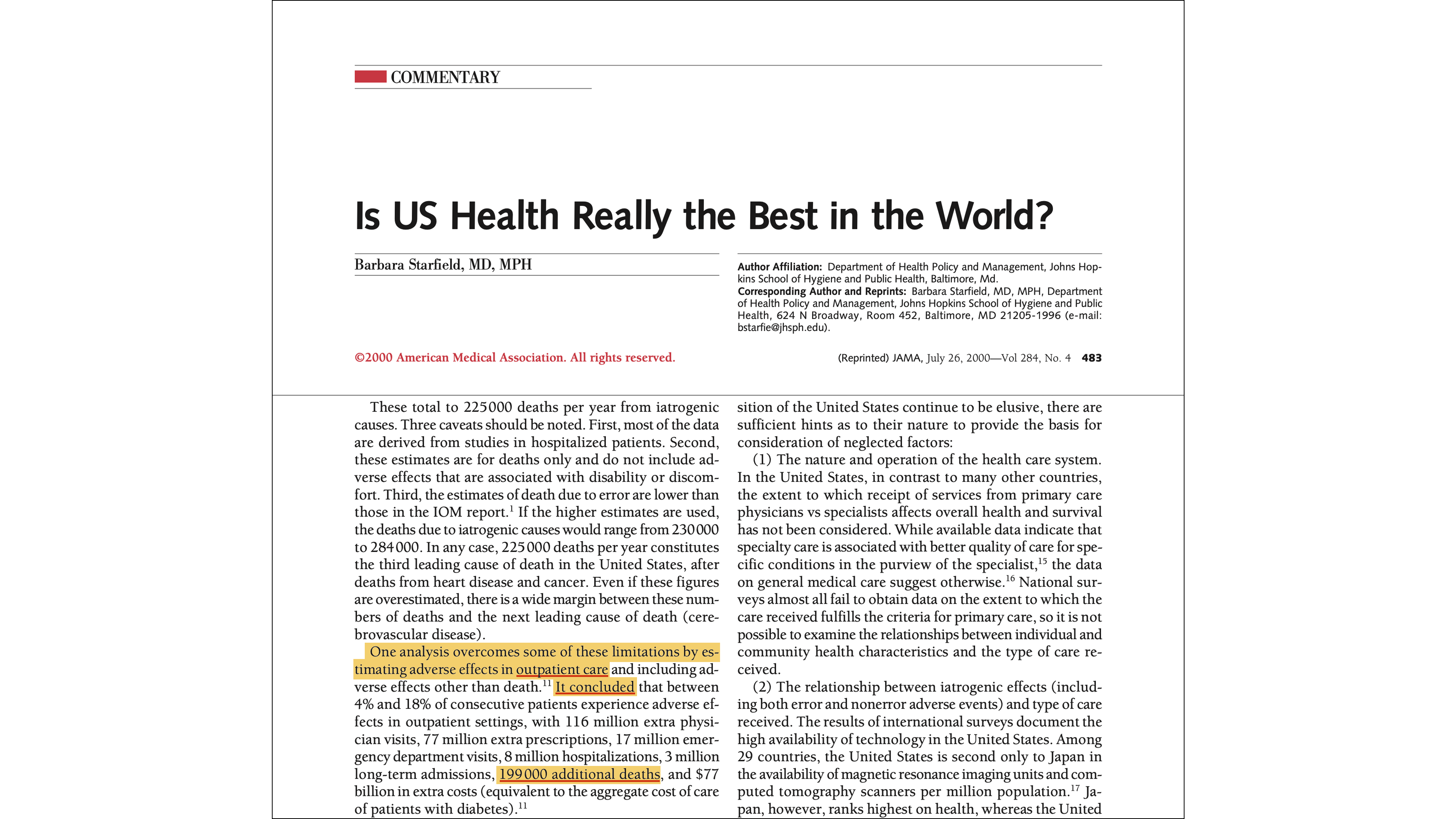
No single paper cleanly isolates the outpatient death toll, but two assessments using the same cost-of-illness model, published decades apart, converge on the same order of magnitude. The original 1995 study estimated approximately 199,000 annual drug-related deaths in the outpatient setting—a figure later cited in a 2000 JAMA analysis of the U.S. health system. A 2018 update subsequently estimated a total of 275,689 deaths from non-optimized drug therapy in both inpatient and outpatient settings combined. Subtract the roughly 128,000 inpatient adverse drug reaction deaths documented in the previous section, and the residual—approximately 148,000 deaths per year—represents the drug-related death toll occurring outside the hospital setting.
Both studies were authored by advocates for expanding clinical pharmacy services. These are not critiques of the pharmaceutical model; they are arguments for more medication management. Yet, by their own math, the outpatient death toll still comes out in the six figures.
Many more deaths beyond the admitted numbers
The half-million-plus deaths tallied above come from the medical system’s own published research—and even those authors admit their estimates are low.
The NIH’s own StatPearls review concedes that only about 1% of serious adverse drug reactions are ever reported to federal regulators. A Harvard study likewise found that less than 0.3% of adverse drug events get reported.
But beyond these acknowledged gaps are entire categories of death that mainstream research will not touch at all—because acknowledging them would implicate core profit centers. These deaths are triple-laundered: excluded from clinical surveillance, miscoded on death certificates, and kept off the research agenda that determines what the public is allowed to know.
Chemotherapy
Chemotherapy is poison. The first chemotherapy drugs were derived from mustard gas—the infamous chemical warfare agent from World War II. It damages tumors, yes, but also everything else. When a cancer patient dies during or shortly after treatment, it’s the chemo that likely killed them—but the death certificate will say cancer.
Vaccines
The vaccine program operates under a liability shield and a cultural taboo that makes honest mortality accounting impossible. Every case of “SIDS” (sudden infant death syndrome) should be investigated as a vaccine reaction—the temporal correlation is overwhelming. Beyond the childhood vaccine schedule, under which American children routinely receive upwards of 70 doses by age 18, the COVID vaccine rollout saw young, healthy people dropping dead from myocarditis and clotting disorders. The system will never properly audit itself here because vaccines are its sacred cow.
Psychiatric drugs
Millions of Americans are kept on psychiatric drugs that damage the body in ways that accumulate over decades—weight gain, organ damage, heart problems—none of which gets attributed to the drugs. These medications can shorten lifespan by decades, but when a patient dies of heart failure at 45, the death certificate says heart disease. The drug they took for 20 years won’t be mentioned. Psychiatry has constructed a feedback loop where the drugs cause deterioration, the deterioration is blamed on mental illness, and more drugs are prescribed.

Death by medical debt
Medical bills are the leading cause of personal bankruptcy in the United States—and financial ruin is a major driver of suicide. The medical system bankrupts people for the privilege of being poisoned. When a man loses his home to cancer bills and puts a gun in his mouth, the death certificate says suicide.
“Brain death”
The “brain death” diagnosis is a conveyor belt to the organ transplant industry. Patients with recoverable conditions are declared dead under protocols that prioritize organ viability over making sure the patient is actually dead. Once that declaration is made, the patient becomes inventory—and the ventilator is turned off on the transplant team’s schedule.

Abortion as “healthcare”
Over a million pregnancies are terminated each year in the U.S. under the banner of healthcare. Whatever one’s position on the ethics, the body count is real.
Euthanasia
Although euthanasia is not legal in the United States (yet), it’s worth mentioning. Where it has been legalized, the eligibility criteria keep expanding. Euthanasia is now the fifth leading cause of death in Canada.

Death rates drop when doctors go on strike
When confronted with the reality that the medical system is the number-one cause of death, people inevitably try to downplay it: “Yes, medicine is dangerous, but it saves far more people than it kills.”
This hypothesis has been tested repeatedly across multiple countries. The pattern is consistent: when doctors go on strike, death rates decline.
In 1976, doctors in Los Angeles County went on strike for five weeks. A study published in the American Journal of Public Health found a significant drop in the county’s mortality rate during that period. When the strike ended, the death rate returned to its pre-strike level. A similar pattern was observed during the 1999 Israeli physician strike, when some local burial societies reported a reduction in deaths of up to 39% over several months. In Bogotá, Colombia, a 52-day doctors’ strike in 1976 produced a 35% decline in the death rate. These are only a few examples.
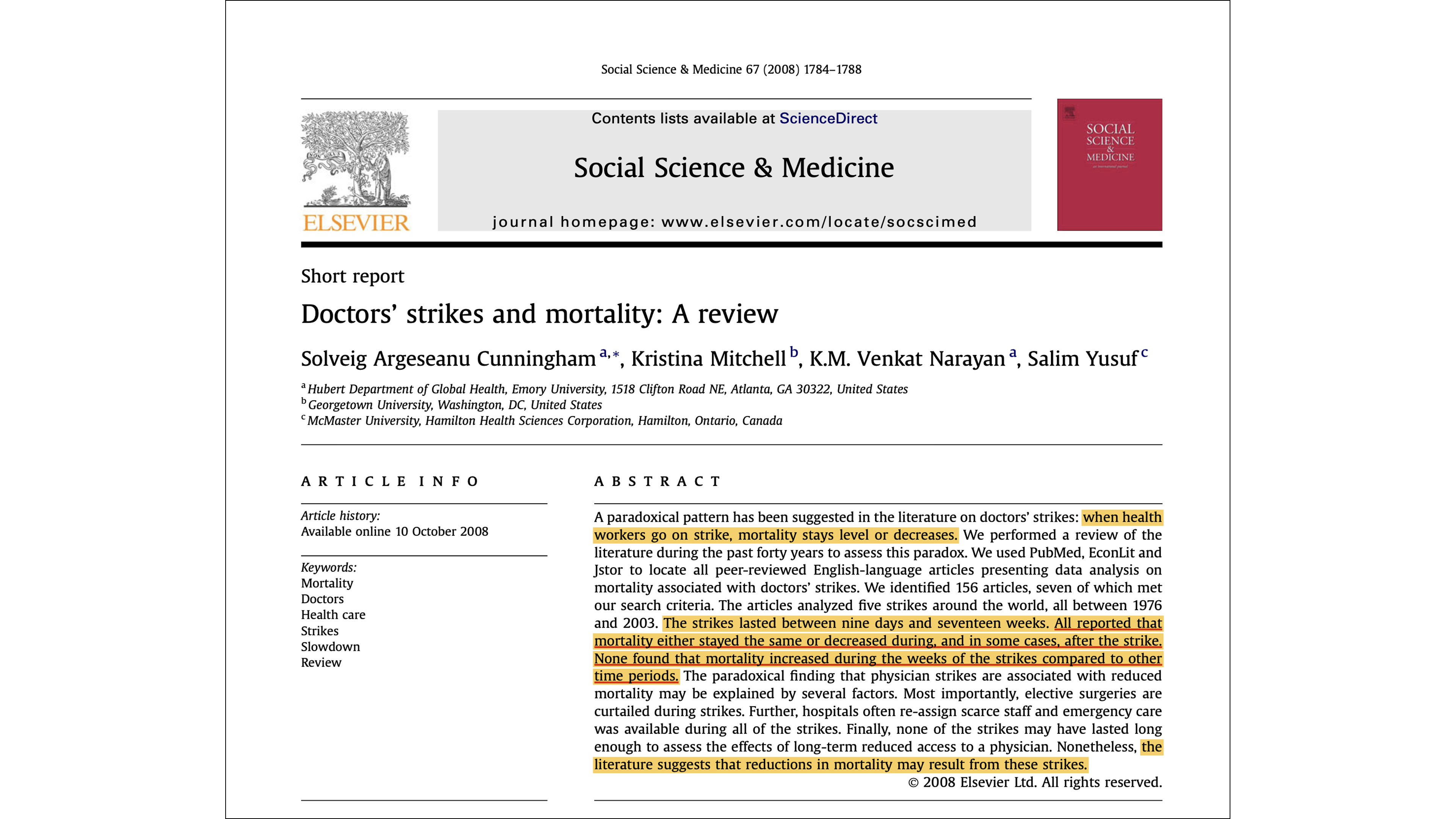
A comprehensive meta-analysis published in 2008 in Social Science & Medicine looked at doctor strikes across several decades and multiple countries. In every case, when medical intervention was reduced, death rates either dropped or stayed the same. They never increased.
It shouldn’t be a mystery why this happens. When doctors stop operating, surgical mistakes stop too. When prescriptions stop, so do harmful drug reactions. And when medical care pauses, so does the harm it causes.
Conclusion
“Doctors will have more lives to answer for in the next world than even we generals.”
—Napoleon Bonaparte
The medical system thrives by turning patients into billable endpoints, launders the deaths it causes through misleading ICD codes, and protects itself with a cultural taboo that makes questioning the “standard of care” tantamount to heresy.
If deaths were accurately re-coded, the tallies for heart disease and cancer would shrink dramatically, and the medical system would be exposed as the leading cause of death.
Until we acknowledge that healthcare is a primary driver of mortality, we will keep looking for answers in the very institutions that profit from our decline.
The Best “Go Paid” Deal on Substack! You Get REAL Stuff!!
Go paid at the $5 a month level, and we will send you both the PDF and e-Pub versions of Etienne’s new book: To See the Cage Is to Leave It - 25 Techniques the Few Use to Control the Many and a coupon code for 10% off anything in the https://artofliberty.org/store/.
Go paid at the $50 a year level, and we will send you a free paperback edition of Etienne’s new book: To See the Cage Is to Leave It - 25 Techniques the Few Use to Control the Many OR “Government” - The Biggest Scam in History… Exposed! OR a 64GB Liberator flash drive if you live in the US. If you are international, we will give you a $10 credit towards shipping if you agree to pay the remainder.
Support us at the $250 Founding Member Level and get a signed high-resolution hardcover of “Government” - The Biggest Scam in History... Exposed! + Liberator flash drive + a signed high-resolution hardcover of Etienne’s new book: To See the Cage Is to Leave It - 25 Techniques the Few Use to Control the Many + everything else in our “Everything Bundle” of the best in voluntaryist thought delivered domestically. International pays shipping. Our only option for signed copies besides catching Etienne @ an event.

Comments ()